This site is intended for healthcare
professionals in Belgium and Luxembourg.
STARTING WITH REBLOZYL®
Reblozyl® should be initiated and monitored under the supervision of a physician experienced in the treatment of hematological diseases.1
START1:
- Hemoglobin (Hb) should be assessed prior to each Reblozyl® administration. In case of a red blood cell (RBC) transfusion occurring prior to dosing, the pre-transfusion Hb level must be considered for dosing purposes
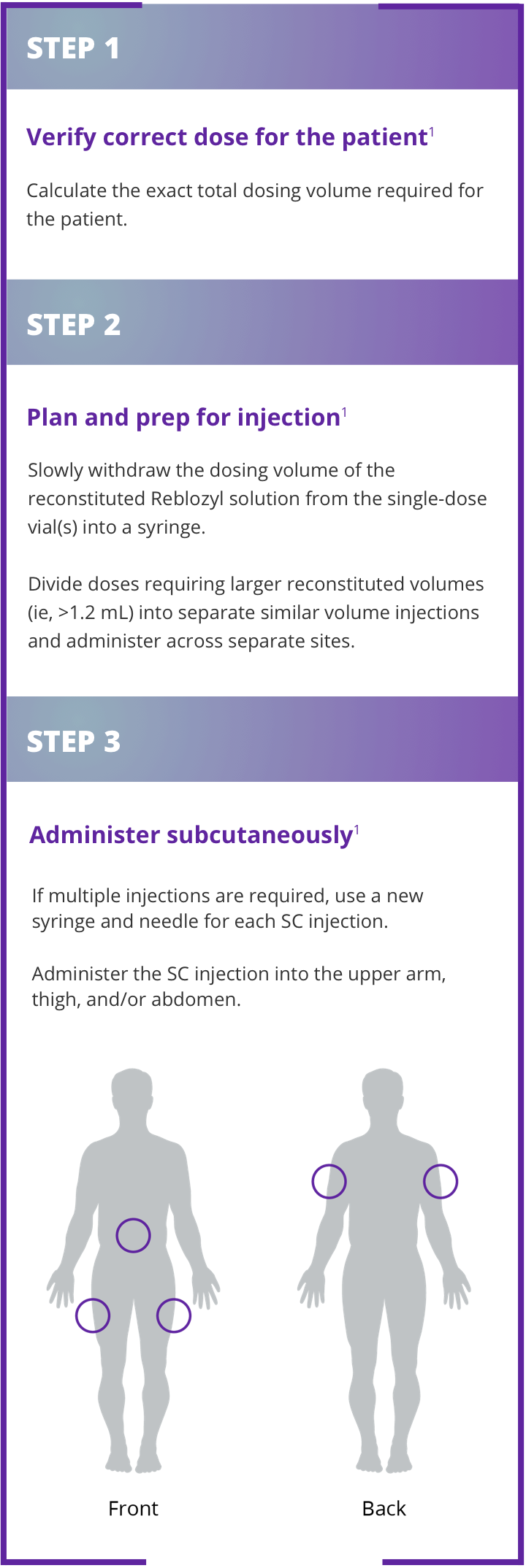
- After reconstitution, Reblozyl® solution should be injected subcutaneously (into the upper arm, thigh or abdomen) every 3 weeks
- The recommended maximum volume of Reblozyl® per injection site is 1.2 mL. With reconstituted volumes larger than 1.2 mL, divide doses into separate similar volume injections and administer across separate injection sites. Reconstitute the appropriate number of Reblozyl vials to achieve the desired dose.
- If a scheduled injection is delayed or missed, administer Reblozyl® as soon as possible and continue dosing as prescribed with at least 3 weeks between doses
- No starting dose adjustments are required in:
- Elderly patients
- Patients with hepatic impairment who have a total bilirubin >upper limit of normal (ULN) and/or alanine aminotransferase or aspartate aminotransferase <3x ULN
- Patients with mild to moderate renal impairment (estimated glomerular filtration rate [eGFR] <90 and ≥30 mL/min/1.73 m2)
MONITOR1:
- If Hb is ≥11.5 g/dL in the absence of transfusions for at least 3 weeks, delay dosing until the Hb is ≤11 g/dL. If there is also a concomitant rapid increase in Hb (>2 g/dL within 3 weeks in absence of transfusion), a dose reduction to one step down (minimum 0.8 mg/kg) should be considered after the dose delay
- If treatment-related Grade 3 or higher adverse reactions occur persistently, delay treatment until toxicity has improved or returned to baseline. After a dose delay, re-start patient at previous dose or at a reduced dose as per dose reduction guidance
- If there is a loss of response to Reblozyl®, assess causative factors (eg, a bleeding event). If typical causes for a loss of hematological response are excluded, consider a dose increase
INDIVIDUALIZE1:
- Dosing is customized by patient response; dosing modifications may be needed
START
- Starting dose is 1.0 mg/kg administered subcutaneously (into the upper arm, thigh, or abdomen) every 3 weeks
- Assess hemoglobin (Hb) prior to each Reblozyl® administration
MONITOR1
- Monitor hemoglobin, adverse drug reactions and loss of clinical benefit, and adapt dosing as needed.
INDIVIDUALIZE
- Dosing is customized by patient response; dosing modifications may be needed
DOSING MODIFICATION
Dosing with Reblozyl® is customized by patient response. The recommended starting dose of Reblozyl® is 1.0 mg/kg once every 3 weeks.1
INCREASE DOSE1:
- Consider a dose increase in patients who are not RBC transfusion-free after at least 2 consecutive administrations (6 weeks) at the prior dose
- The dose increase should not occur more frequently than every 6 weeks (2 administrations) and should not exceed the maximum dose of 1.75 mg/kg every 3 weeks. The dose should not be increased immediately after a dose delay. For patients with a pre-dose Hb level of > 9 g/dL and who have not yet achieved transfusion independence, a dose increase may be required at the physician’s discretion; the risk of Hb increasing above the target threshold with concomitant transfusion cannot be excluded
- If a patient loses response to Reblozyl® (ie, transfusion independence), increase dose by one dose level
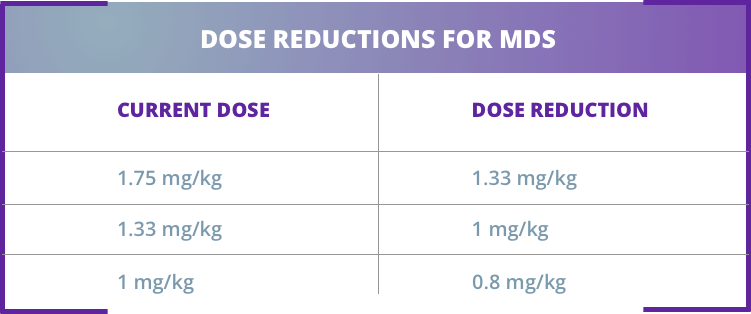
REDUCE DOSE1:
- In case of Hb increase ≥2 g/dL within 3 weeks, in absence of transfusions, reduce Reblozyl® dose by one dose level1
- If the Hb is ≥11.5 g/dL in the absence of transfusion for at least 3 weeks, the dose should be delayed until the Hb is ≤11.0 g/dL
- If there is also a concomitant rapid increase in Hb (> 2 g/dL within 3 weeks in absence of transfusion), a dose reduction to one step down (minimum 0.8 mg/kg) should be considered after the dose delay
- Dose should not be reduced below 0.8 mg/kg
DISCONTINUE1:
- Reblozyl® should be discontinued if patients do not experience a reduction in transfusion burden after 9 weeks of treatment (3 doses) at the maximum dose level if no alternative explanations for response failure are found (e.g. bleeding, surgery, other concomitant illnesses) or if unacceptable toxicity occurs at any time
Reblozyl® offers stepwise dose increases to achieve
individual patient response1
INCREASE DOSE1:

The dose should not be increased more frequently than every 6 weeks (2 doses) and should not exceed the maximum dose of 1.75 mg/kg every 3 weeks. The dose should not be increased immediately after a dose delay.1
REDUCE DOSE1:
DISCONTINUE1:
PREPARATION & ADMINISTRATION
Reconstitution1
Reblozyl® must be reconstituted gently prior to administration. Aggressive shaking should be avoided.
The appropriate number of Reblozyl® vials should be reconstituted to achieve the desired dose. A syringe with appropriate graduations must be used for reconstitution to ensure accurate dosage.
After reconstitution, each mL of solution contains 50 mg of Reblozyl®. Any unused medicinal product or waste material should be disposed of in accordance with local requirements.1
Download the Dosing &
Administration Guides.
These guides include all the information found here, as well as the full steps for reconstitution of Reblozyl®, plus storage information:
- Reconstitution Guide (French)
- Reconstitution Guide (Dutch)
- Administration Guide (French)
- Administration Guide (Dutch)
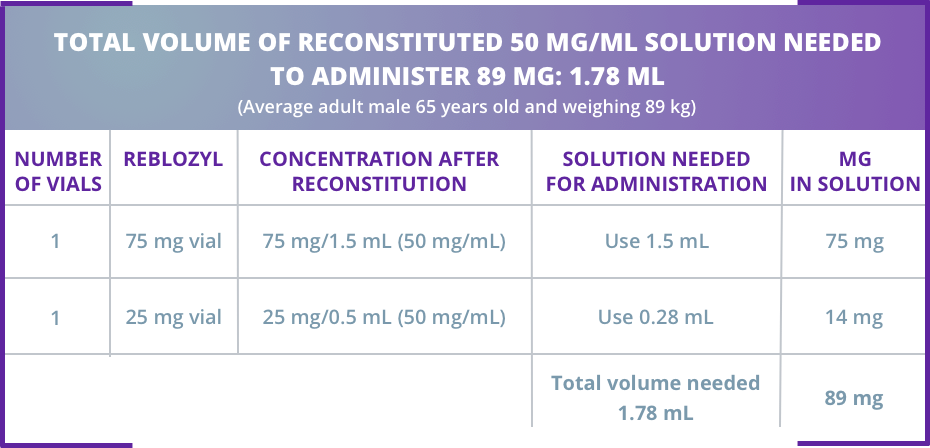
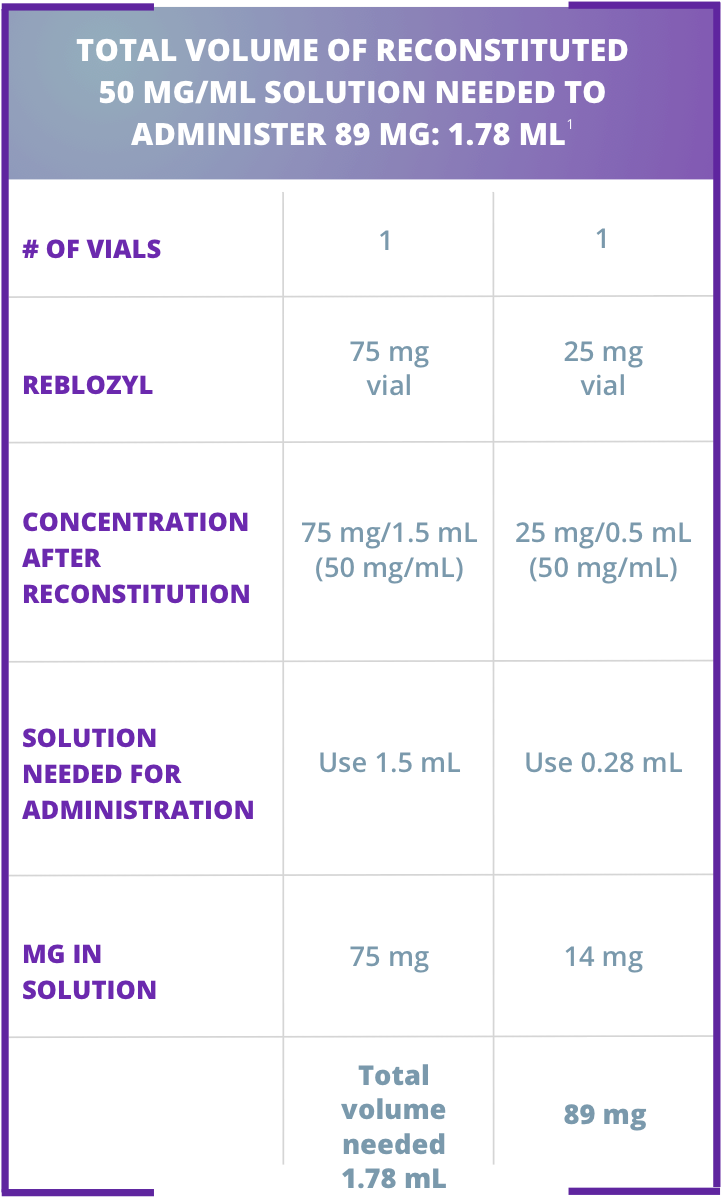
Sample calculation for subcutaneous administration of Reblozyl®
- Average adult male 65 years old and weighing 89 kg
- 1 mg of Reblozyl® per 1 kg = 89 mg starting dose
Administering Reblozyl®1
- Prior to administration, allow solution to reach room temperature for a more comfortable injection
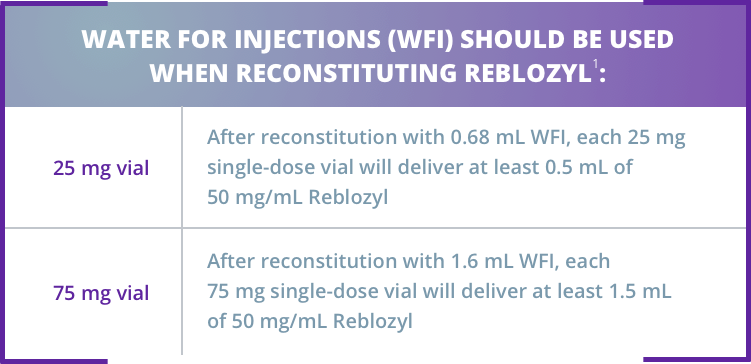
Reblozyl® is available in 2 strengths as single-dose vials for reconstitution1
Reblozyl® is supplied as a lyophilized powder for reconstitution before use
Sample calculation for subcutaneous administration of Reblozyl®
Dividing doses and administering with reconstituted volumes larger than 1.2 mL:1
Injection 1: 0.89 mL – in upper arm Injection 2: 0.89 mL – in thigh or abdomen
Reblozyl® is administered subcutaneously every 3 weeks1
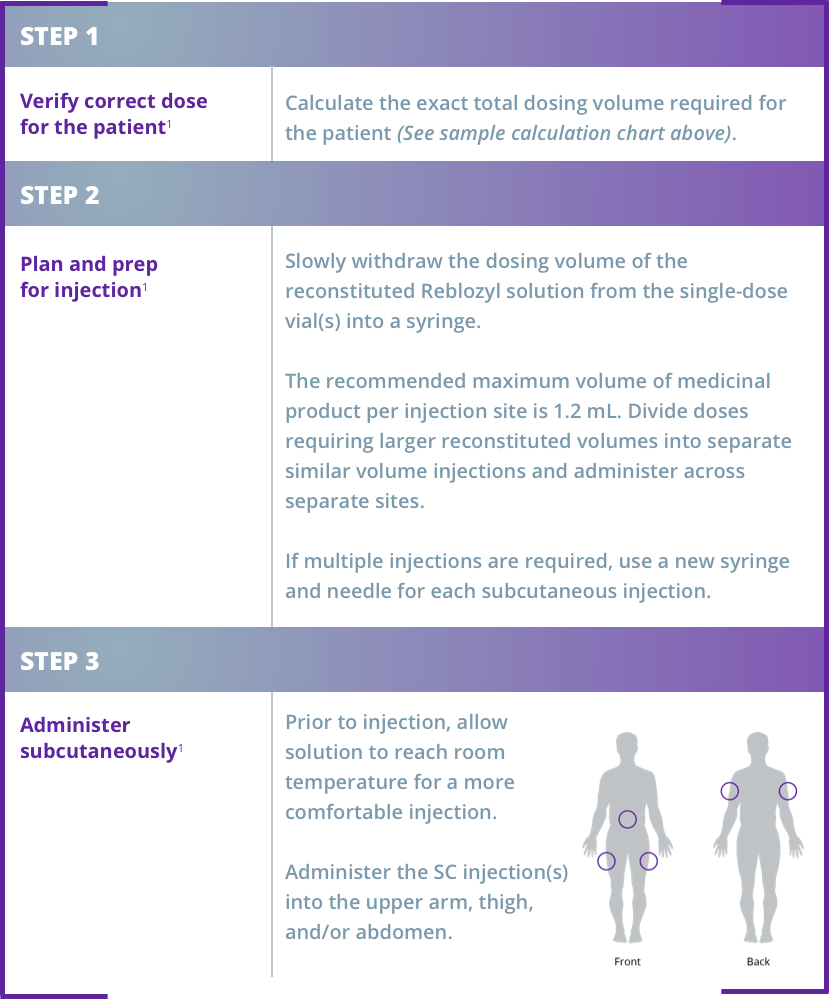
Do not administer more than 1 dose from a vial
Do not mix with other medications
Do not pool unused portions from the vials
Discard any unused portion
Reblozyl® should be initiated and monitored under the supervision of a physician experienced in the treatment of hematological diseases.1
START1:
- Hemoglobin (Hb) should be assessed prior to each Reblozyl® administration. In case of a red blood cell (RBC) transfusion occurring prior to dosing, the pre-transfusion Hb level must be considered for dosing purposes
- After reconstitution, Reblozyl® solution should be injected subcutaneously (into the upper arm, thigh or abdomen) every 3 weeks
- The recommended maximum volume of Reblozyl® per injection site is 1.2 mL. With reconstituted volumes larger than 1.2 mL, divide doses into separate similar volume injections and administer across separate injection sites. Reconstitute the appropriate number of Reblozyl vials to achieve the desired dose.
- If a scheduled injection is delayed or missed, administer Reblozyl® as soon as possible and continue dosing as prescribed with at least 3 weeks between doses
- No starting dose adjustments are required in:
- Elderly patients
- Patients with hepatic impairment who have a total bilirubin >upper limit of normal (ULN) and/or alanine aminotransferase or aspartate aminotransferase <3x ULN
- Patients with mild to moderate renal impairment (estimated glomerular filtration rate [eGFR] <90 and ≥30 mL/min/1.73 m2)
MONITOR1:
- If Hb is ≥11.5 g/dL in the absence of transfusions for at least 3 weeks, delay dosing until the Hb is ≤11 g/dL. If there is also a concomitant rapid increase in Hb (>2 g/dL within 3 weeks in absence of transfusion), a dose reduction to one step down (minimum 0.8 mg/kg) should be considered after the dose delay
- If treatment-related Grade 3 or higher adverse reactions occur persistently, delay treatment until toxicity has improved or returned to baseline. After a dose delay, re-start patient at previous dose or at a reduced dose as per dose reduction guidance
- If there is a loss of response to Reblozyl®, assess causative factors (eg, a bleeding event). If typical causes for a loss of hematological response are excluded, consider a dose increase
INDIVIDUALIZE1:
- Dosing is customized by patient response; dosing modifications may be needed
Dosing with Reblozyl® is customized by patient response. The recommended starting dose of Reblozyl® is 1.0 mg/kg once every 3 weeks.1
Reblozyl® offers stepwise dose increases to achieve individual patient response1
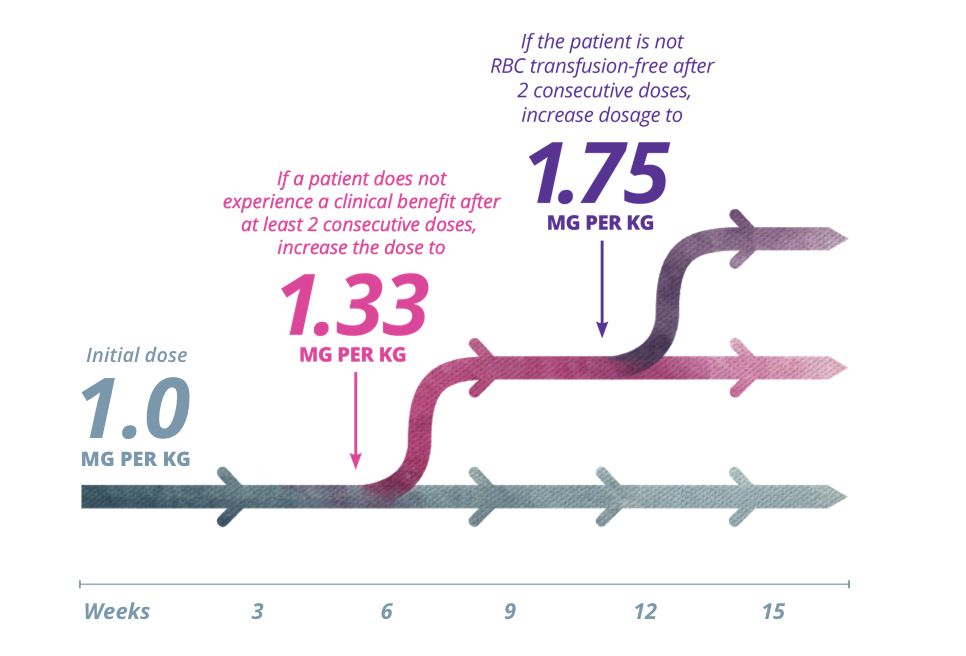
The dose should not be increased more frequently than every 6 weeks (2 doses) and should not exceed the maximum dose of 1.75 mg/kg every 3 weeks. The dose should not be increased immediately after a dose delay.1
INCREASE DOSE1:
- Consider a dose increase in patients who are not RBC transfusion-free after at least 2 consecutive administrations (6 weeks) at the prior dose
- The dose increase should not occur more frequently than every 6 weeks (2 administrations) and should not exceed the maximum dose of 1.75 mg/kg every 3 weeks. The dose should not be increased immediately after a dose delay. For patients with a pre-dose Hb level of > 9 g/dL and who have not yet achieved transfusion independence, a dose increase may be required at the physician’s discretion; the risk of Hb increasing above the target threshold with concomitant transfusion cannot be excluded
- If a patient loses response to Reblozyl® (ie, transfusion independence), increase dose by one dose level
REDUCE DOSE1:
- In case of Hb increase ≥2 g/dL within 3 weeks, in absence of transfusions, reduce Reblozyl® dose by one dose level1
- If the Hb is ≥11.5 g/dL in the absence of transfusion for at least 3 weeks, the dose should be delayed until the Hb is ≤11.0 g/dL
- If there is also a concomitant rapid increase in Hb (> 2 g/dL within 3 weeks in absence of transfusion), a dose reduction to one step down (minimum 0.8 mg/kg) should be considered after the dose delay
- Dose should not be reduced below 0.8 mg/kg
DISCONTINUE1:
- Reblozyl® should be discontinued if patients do not experience a reduction in transfusion burden after 9 weeks of treatment (3 doses) at the maximum dose level if no alternative explanations for response failure are found (e.g. bleeding, surgery, other concomitant illnesses) or if unacceptable toxicity occurs at any time
Reblozyl® is available in 2 strengths as single-dose vials for reconstitution1
- Reblozyl® is supplied as a lyophilized powder for reconstitution before use
Reblozyl® must be reconstituted gently prior to administration. Aggressive shaking should be avoided.
The appropriate number of Reblozyl® vials should be reconstituted to achieve the desired dose. A syringe with appropriate graduations must be used for reconstitution to ensure accurate dosage.
After reconstitution, each mL of solution contains 50 mg of Reblozyl®. Any unused medicinal product or waste material should be disposed of in accordance with local requirements.1
Download the Dosing & Administration Guides.
These guides include all the information found here, as well as the full steps for reconstitution of Reblozyl®, plus storage information:
- Average adult male 65 years old and weighing 89 kg
- 1 mg of Reblozyl® per 1 kg = 89 mg starting dose
Dividing doses and administering with reconstituted volumes larger than 1.2 mL:1
Injection 1: 0.89 mL – in upper arm
Injection 2: 0.89 mL – in thigh or abdomen
Reblozyl® is administered subcutaneously every 3 weeks1
- Prior to administration, allow solution to reach room temperature for a more comfortable injection
Do not administer more than 1 dose from a vial
Do not mix with other medications
Do not pool unused portions from the vials
Discard any unused portion