This site is intended for healthcare
professionals in Belgium and Luxembourg.
WHY IPSS-R
The IPSS-R provides a more accurate prognosis in terms of overall survival and evolution to acute myeloid leukemia compared with the IPSS.2
The IPSS-R accounts for:
- 5 major prognostic categories, rather than 4 as in the IPSS2
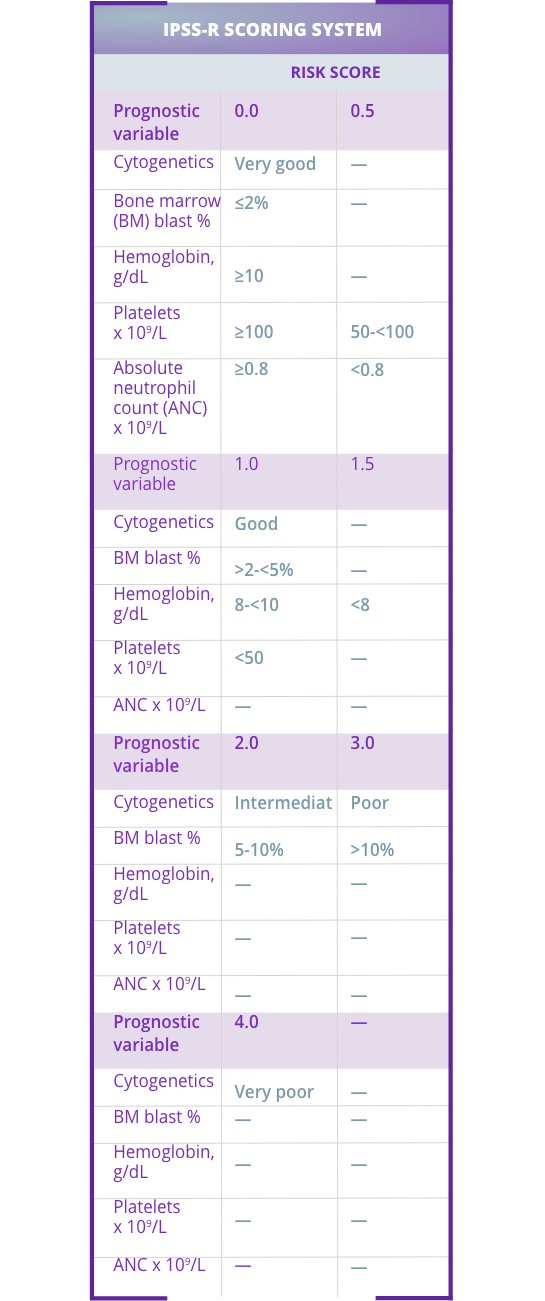
- Cytogenetic risk groups, marrow blast percentage, and depth of cytopenias (hemoglobin, platelet and absolute neutrophil count levels)2
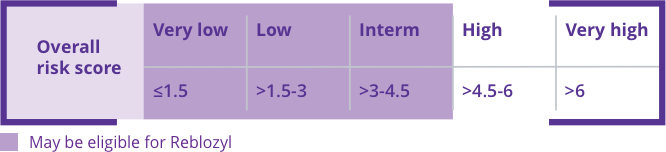
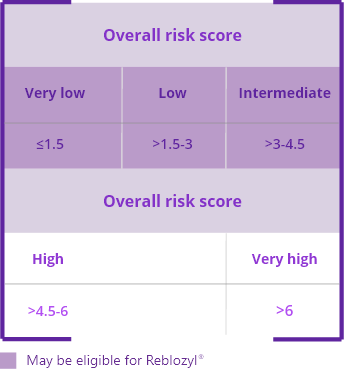
The International Prognosis Scoring System-Revised (IPSS-R) helps identify very low- to intermediate-risk patients who may be eligible for Reblozyl®.1,2

DETERMINING
RS STATUS
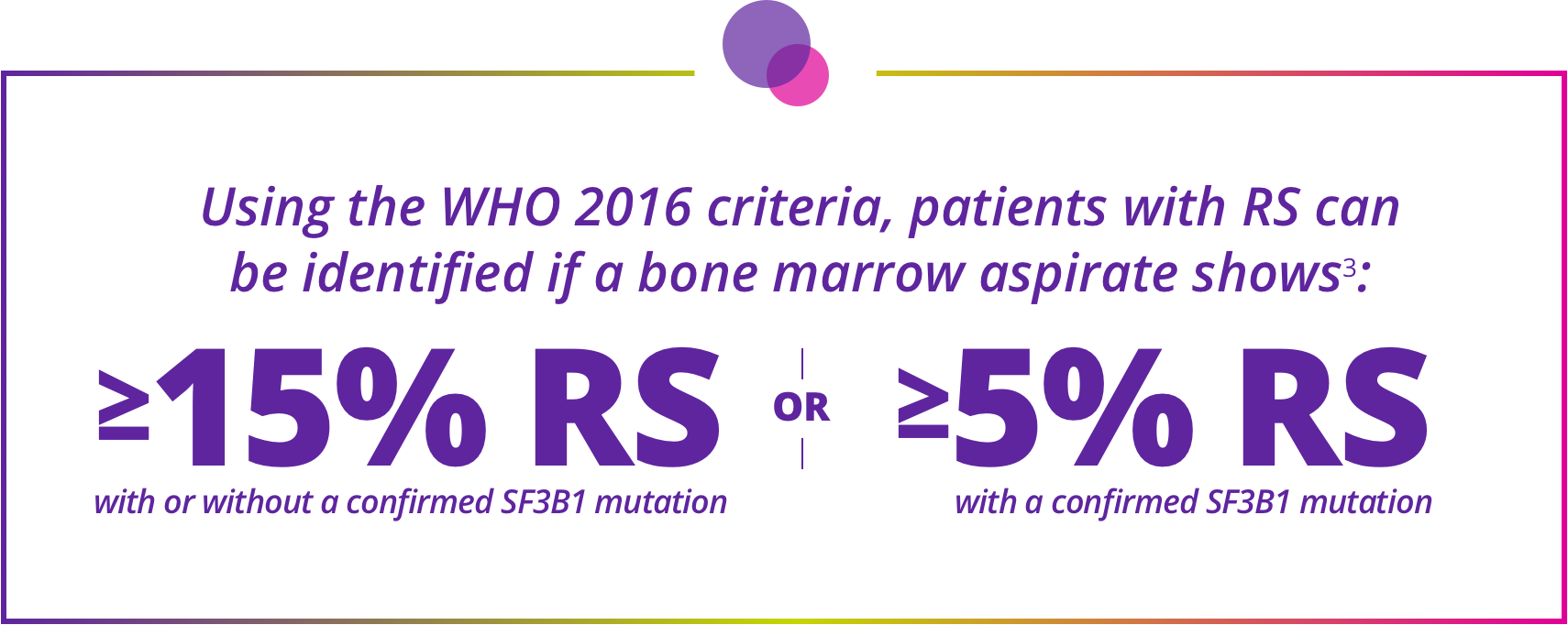
Staining for RS and checking for SF3B1 mutations are needed to accurately classify MDS using WHO 2016 criteria.3
- Staining for RS should be done routinely on initial evaluation4
- RS are identified through Perls’ staining, which can be easily performed, even on samples that have been previously stored5,6
Determining ring sideroblast (RS) status is essential for accurate classification of MDS subtypes and patient eligibility for Reblozyl®3
ESA RESPONSE
STATUS
There is an unmet clinical need for patients who have an unsatisfactory response to or are ineligible for erythropoiesis-stimulating agents (ESAs)7-8
- Selection criteria for ESAs include endogenous EPO levels of <500 mU/mL but, in an ESA registration trial, no patients with endogenous EPO levels of ≥200 mU/mL had a response8,10,11
Primary ESA resistance is more frequent among patients with MDS-RS vs MDS without RS, while durable responses are less frequent9,12
- According to IWG 2006 Criteria for Hematological Improvement an adequate response includes a hemoglobin increase by at least 1.5 g/dL or a reduction in RBC transfusions by at least 4 transfusions in 8 weeks13
- An effect must persist at least 8 weeks to be considered a response13

CONTRAINDICATIONS OF REBLOZYL®
Pregnancy
Treatment with Reblozyl® should not be started if the woman is pregnant. There are no data from the use of Reblozyl® in pregnant women. Studies in animals have shown reproductive toxicity.
Women of childbearing potential should use effective contraception during treatment with Reblozyl® and for at least 3 months after the last dose.
Prior to starting treatment with Reblozyl®, a pregnancy test should be performed for women of childbearing potential.
If a patient becomes pregnant, Reblozyl® should be discontinued.
Contraindications1
PREGNANCY
HYPERSENSITIVITY
to the active substance or to any of the excipients
Please consult the full summary of Product Characteristics (SmPC) before prescribing: SmPC in French, SmPC in Dutch.
SPECIAL
WARNINGS AND
PRECAUTIONS
Traceability
In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded.
Increased blood pressure
In controlled clinical studies in MDS and β-thalassemia, patients treated with Reblozyl® had an average increase in systolic and diastolic blood pressure of 5 mm Hg from baseline not observed in patients receiving placebo. Blood pressure should be monitored prior to each Reblozyl® administration. In the case of persistent hypertension or exacerbations of pre-existing hypertension, patients should be treated for hypertension as per current clinical guidelines.
Sodium content
This medicinal product contains less than 1 mmol sodium (23 mg) per dose, that is to say it is essentially “sodium-free.”
TRACEABILITY
Record the name and batch number of Reblozyl®
THROMBOEMBOLIC EVENTS
The occurrence of TEE was not correlated with elevated
hemoglobin levels
INCREASED BLOOD PRESSURE
Monitor blood pressure prior to administering Reblozyl®
SODIUM CONTENT
Reblozyl® is essentially “sodium-free”
The International Prognosis Scoring System-Revised (IPSS-R) helps identify very low- to intermediate-risk patients who may be eligible for Reblozyl®.1,2
The IPSS-R provides a more accurate prognosis in terms of overall survival and evolution to acute myeloid leukemia compared with the IPSS.2
The IPSS-R accounts for:
- 5 major prognostic categories, rather than 4 as in the IPSS2
- Cytogenetic risk groups, marrow blast percentage, and depth of cytopenias (hemoglobin, platelet and absolute neutrophil count levels)2
Determining ring sideroblast (RS) status is essential for accurate classification of MDS subtypes and patient eligibility for Reblozyl®3
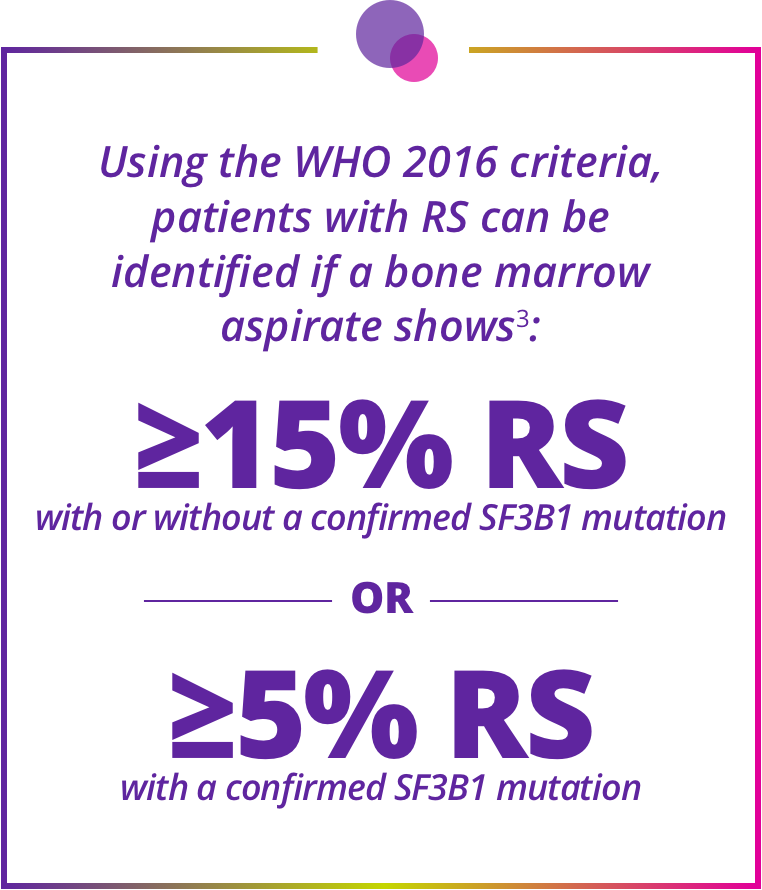
Staining for RS and checking for SF3B1 mutations are needed to accurately classify MDS using WHO 2016 criteria.
- Staining for RS should be done routinely on initial evaluation4
- RS are identified through Perls’ staining, which can be easily performed, even on samples that have been previously stored 5,6
There is an unmet clinical need for patients who have an unsatisfactory response to or are ineligible for erythropoiesis-stimulating agents (ESAs)7-8
- Selection criteria for ESAs include endogenous EPO levels of <500 mU/mL but, in an ESA registration trial, no patients with endogenous EPO levels of ≥200 mU/mL had a response8,10,11
- Primary ESA resistance is more frequent among patients with MDS-RS vs MDS without RS, while durable responses are less frequent9,12
- According to IWG 2006 Criteria for Hematological Improvement an adequate response includes a hemoglobin increase by at least 1.5 g/dL or a reduction in RBC transfusions by at least 4 transfusions in 8 weeks13
- An effect must persist at least 8 weeks to be considered a response13
- ESAs are used widely and are most effective in patients with low RBC transfusion requirements, a low serum EPO level, and lower-risk MDS per the IPSS-R9,10
- Many patients are unresponsive to, or lose response to, ESAs9
- Once ESAs fail, many patients rely on RBC transfusions, which are associated with reduced overall survival and burdensome complications7,9,14,15
- Patients, therefore, need an effective treatment option that could reduce dependence on RBC transfusions10
Contraindications1
PREGNANCY
HYPERSENSITIVITY
to the active substance or to any of the excipients
Pregnancy
Treatment with Reblozyl® should not be started if the woman is pregnant. There are no data from the use of Reblozyl® in pregnant women. Studies in animals have shown reproductive toxicity.
Women of childbearing potential should use effective contraception during treatment with Reblozyl® and for at least 3 months after the last dose.
Prior to starting treatment with Reblozyl®, a pregnancy test should be performed for women of childbearing potential.
If a patient becomes pregnant, Reblozyl® should be discontinued.
Please consult the full summary of Product Characteristics (SmPC) before prescribing: SmPC in French, SmPC in Dutch.
TRACEABILITY
In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded.
THROMBOEMBOLIC EVENTS
The occurrence of TEE was not correlated with elevated hemoglobin levels
INCREASED BLOOD PRESSURE
In controlled clinical studies in MDS and β-thalassemia, patients treated with Reblozyl® had an average increase in systolic and diastolic blood pressure of 5 mm Hg from baseline not observed in patients receiving placebo. Blood pressure should be monitored prior to each Reblozyl® administration. In the case of persistent hypertension or exacerbations of pre-existing hypertension, patients should be treated for hypertension as per current clinical guidelines.
SODIUM CONTENT
This medicinal product contains less than 1 mmol sodium (23 mg) per dose, that is to say it is essentially “sodium-free.”